Genetics FAQs
What is Alpha-1 Antitrypsin Deficiency?
Alpha-1 antitrypsin deficiency (Alpha-1, AATD) is an inherited condition that raises the risk for lung disease. Risk for liver disease is also increased in many people with Alpha-1. Lung disease typically occurs in adulthood, while liver disease can occur in children or adults. People with Alpha-1 do not produce a protein called alpha-1 antitrypsin normally.
Alpha-1 antitrypsin is a protein that is made in the liver. It is then secreted into the blood. Alpha-1 antitrypsin is needed in circulation to protect the lungs. Without enough of it, the lungs are at risk to develop chronic obstructive pulmonary disease ( COPD ).
The way each person's body makes Alpha-1 antitrypsin is determined by genes. Everyone has two copies of the alpha-1 gene, one inherited from each parent. Abnormal Alpha-1 genes result in Alpha-1 deficiency. The “Z” mutation produces abnormal alpha-1 antitrypsin that builds up in the liver, rather than passing into circulation. People with two Z genes (ZZ) have high lifetime risks for lung and liver disease. There are other mutations that can cause Alpha-1, too. For example, the S, F, and I mutations are different abnormal versions of the gene. The normal gene for Alpha-1 is called “M”. MM is the normal gene combination.
Alpha-1 is an inherited risk. Not everyone with Alpha-1 will develop symptoms, or the same symptoms. It is important to know about Alpha-1 because there are ways to reduce risks (such as avoiding smoking), and medical care to detect and treat symptoms for better outcomes. For people with Alpha-1 COPD, a specific therapy, called augmentation therapy, may be recommended. Because Alpha-1 genes run in families, knowing about Alpha-1 can be important for relatives and family planning.
Alpha-1 antitrypsin is a protein that is made in the liver. It is then secreted into the blood. Alpha-1 antitrypsin is needed in circulation to protect the lungs. Without enough of it, the lungs are at risk to develop chronic obstructive pulmonary disease ( COPD ).
The way each person's body makes Alpha-1 antitrypsin is determined by genes. Everyone has two copies of the alpha-1 gene, one inherited from each parent. Abnormal Alpha-1 genes result in Alpha-1 deficiency. The “Z” mutation produces abnormal alpha-1 antitrypsin that builds up in the liver, rather than passing into circulation. People with two Z genes (ZZ) have high lifetime risks for lung and liver disease. There are other mutations that can cause Alpha-1, too. For example, the S, F, and I mutations are different abnormal versions of the gene. The normal gene for Alpha-1 is called “M”. MM is the normal gene combination.
Alpha-1 is an inherited risk. Not everyone with Alpha-1 will develop symptoms, or the same symptoms. It is important to know about Alpha-1 because there are ways to reduce risks (such as avoiding smoking), and medical care to detect and treat symptoms for better outcomes. For people with Alpha-1 COPD, a specific therapy, called augmentation therapy, may be recommended. Because Alpha-1 genes run in families, knowing about Alpha-1 can be important for relatives and family planning.
What are genes?
Genes are the genetic “blueprint” for how our bodies develop and function. Genes are units of DNA. People have about 20,000 genes. They are found inside the nucleus of our cells. Genes are passed from parent to child. People get one copy of each gene from their mother and one from their father (sex chromosome genes excluded).
Everyone has changes in their genes that make them unique. Changes in genes can be neutral variants or cause problems. Changes that cause disease or raise risks are called pathogenic variants or mutations. Mutations in one specific gene cause Alpha-1 deficiency. The gene for Alpha-1 is called SERPINA1.
Everyone has changes in their genes that make them unique. Changes in genes can be neutral variants or cause problems. Changes that cause disease or raise risks are called pathogenic variants or mutations. Mutations in one specific gene cause Alpha-1 deficiency. The gene for Alpha-1 is called SERPINA1.
What are alleles?
Alleles are different versions of the same gene. The normal Alpha-1 allele is called "M." Abnormal allelles, also called pathogenic variants or mutations, occur due to changes in the DNA of the Alpha-1 gene that affect how Alpha-1 is made. Mutations result in an abnormal quantity and/or abnormal function of alpha-1 antitrypsin.
The most common deficiency alleles are "S" and "Z." There are also more than 100 other rarer deficiency alleles (such as F and I and null alleles). The M allele (M1, M2, M3) produces normal Alpha-1 protein (normal quantity and normal function). Different deficiency alleles have different effects on Alpha-1 level and function, thus different allele combinations (genotypes) lead to different disease risks. %b M - The M allele is normal (normal alpha-1 antitrypsin quantity and function).
F – The F mutation produces a dysfunctional alpha-1 protein product.
Z - The Z mutation produces an abnormal protein product that gets trapped in the liver and reduces the quantity of alpha-1 antitrypsin (AAT) in the blood.
S - The S mutation causes a moderate reduction in the quantity of alpha-1 antitrypsin (AAT) in the blood.
I - The I mutation results in a reduced quantity of Alpha-1 protein in the blood.
Null - Null mutations make no alpha-1 antitrypsin (AAT); no AAT is produced in the liver or found in the blood as a result of null mutations. There are many different null mutations.
Rare - Rare mutations may make altered forms of alpha-1 antitrypsin (AAT). There are many different rare mutations. Most rare mutations reduce the quantity of alpha-1 antitrypsin (AAT) in the blood. A few rare mutations cause alpha-1 trapping in the liver or altered alpha-1 function.
The most common deficiency alleles are "S" and "Z." There are also more than 100 other rarer deficiency alleles (such as F and I and null alleles). The M allele (M1, M2, M3) produces normal Alpha-1 protein (normal quantity and normal function). Different deficiency alleles have different effects on Alpha-1 level and function, thus different allele combinations (genotypes) lead to different disease risks. %b M - The M allele is normal (normal alpha-1 antitrypsin quantity and function).
F – The F mutation produces a dysfunctional alpha-1 protein product.
Z - The Z mutation produces an abnormal protein product that gets trapped in the liver and reduces the quantity of alpha-1 antitrypsin (AAT) in the blood.
S - The S mutation causes a moderate reduction in the quantity of alpha-1 antitrypsin (AAT) in the blood.
I - The I mutation results in a reduced quantity of Alpha-1 protein in the blood.
Null - Null mutations make no alpha-1 antitrypsin (AAT); no AAT is produced in the liver or found in the blood as a result of null mutations. There are many different null mutations.
Rare - Rare mutations may make altered forms of alpha-1 antitrypsin (AAT). There are many different rare mutations. Most rare mutations reduce the quantity of alpha-1 antitrypsin (AAT) in the blood. A few rare mutations cause alpha-1 trapping in the liver or altered alpha-1 function.
What are genotypes?
A genotype is the combination of Alpha-1 alleles you have. The normal genotype is MM (two copies of the normal M allele). Carrier genotypes include MS, MZ, MF, MI, Mnull and other genotypes where one allele is a normal M and the other is abnormal.
Deficiency genotypes include ZZ, SZ, FZ, IZ, Znull and some others where a person has two abnormal genes.
There are many more rare Alpha-1 genotypes.
Deficiency genotypes include ZZ, SZ, FZ, IZ, Znull and some others where a person has two abnormal genes.
There are many more rare Alpha-1 genotypes.
How does Alpha-1 run in families?
Everyone has two copies of the Alpha-1 gene. Severe deficiency (low levels) of alpha-1 antitrypsin occurs when both copies have a mutation. A mild deficiency, or intermediate alpha-1 antitrypsin level, may occur in carriers with one abnormal gene.
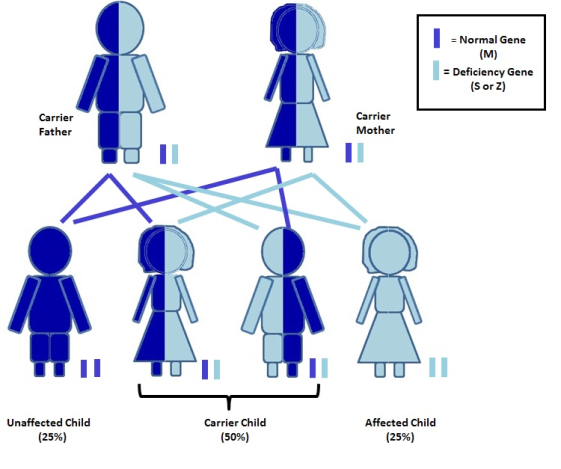
Genes are inherited. We get one copy of the Alpha-1 gene from our mother and the other from our father. If you have children, you pass on one of your two Alpha-1 genes, and the child gets their second Alpha-1 gene from the other parent. When both parents have one or more abnormal Alpha-1 genes there is a risk to have a child with severe deficiency.
Genes are inherited. We get one copy of the Alpha-1 gene from our mother and the other from our father. If you have children, you pass on one of your two Alpha-1 genes, and the child gets their second Alpha-1 gene from the other parent. When both parents have one or more abnormal Alpha-1 genes there is a risk to have a child with severe deficiency.
What does it mean to be a carrier?
People who have one normal Alpha-1 gene (called M) and one abnormal Alpha-1 gene (S,Z, F, I, other) are often called carriers. Carrier genotypes include MS, MZ, MF, MI, M-Other.
Carriers may be termed “mildly deficient” because this combination of genes leads to a lower Alpha-1 level than expected for most people with two normal genes (MM) but higher than that of someone with severe deficiency caused by two abnormal genes (ZZ, SZ).
Most carriers do not develop Alpha-1 related symptoms; however, recent research has shown that MZ carriers who smoke are at high risk for COPD. MZ carriers also have a small increased risk for liver disease. Carriers should avoid smoking and live a healthy lifestyle.
There are over 20 million Alpha-1 carriers in the US. Being an Alpha-1 carrier is more common than many people know. About 2-3% of North Americans are carriers of the Z mutation (MZ) and about 5% carry the S (MS). Carriers of other mutations such as the F, I, and rare/null mutations are less common and exact rates are not known. A person's individual chance to be a carrier depends on their ethnic background and family history.
The good news is that most carriers never have health problems due to their Alpha-1 mutation. However, research continues to better define select groups of people with higher risk for COPD. It is possible that certain carrier sub-groups with higher risk will be defined in the future. Any person experiencing symptoms or a change in their health should see a healthcare provider for personal evaluation.
Carriers have a 50% chance of passing on their abnormal Alpha-1 gene to each child, so, any child of a carrier has a 50% chance to be a carrier, too. If two carriers have children together, there is a risk to have a child with severe Alpha-1 antitrypsin deficiency. This happens when the child inherits an abnormal gene from both the mother and the father.
Carriers may be termed “mildly deficient” because this combination of genes leads to a lower Alpha-1 level than expected for most people with two normal genes (MM) but higher than that of someone with severe deficiency caused by two abnormal genes (ZZ, SZ).
Most carriers do not develop Alpha-1 related symptoms; however, recent research has shown that MZ carriers who smoke are at high risk for COPD. MZ carriers also have a small increased risk for liver disease. Carriers should avoid smoking and live a healthy lifestyle.
There are over 20 million Alpha-1 carriers in the US. Being an Alpha-1 carrier is more common than many people know. About 2-3% of North Americans are carriers of the Z mutation (MZ) and about 5% carry the S (MS). Carriers of other mutations such as the F, I, and rare/null mutations are less common and exact rates are not known. A person's individual chance to be a carrier depends on their ethnic background and family history.
The good news is that most carriers never have health problems due to their Alpha-1 mutation. However, research continues to better define select groups of people with higher risk for COPD. It is possible that certain carrier sub-groups with higher risk will be defined in the future. Any person experiencing symptoms or a change in their health should see a healthcare provider for personal evaluation.
Carriers have a 50% chance of passing on their abnormal Alpha-1 gene to each child, so, any child of a carrier has a 50% chance to be a carrier, too. If two carriers have children together, there is a risk to have a child with severe Alpha-1 antitrypsin deficiency. This happens when the child inherits an abnormal gene from both the mother and the father.
What is a Pi type?
Pi stands for Protease Inhibitor. Alpha-1 antitrypsin is a type of protein called a protease inhibitor, so Pi type is the type(s) of Alpha-1 protein produced by your body (in your liver).
The normal Pi type is M. Normal M variants include M1, M2 and M3. Abnormal Pi types included Z, S, F, I and others.
In most cases your Pi type and your genotype are the same since the genes instruct the type of alpha-1 antitrypsin your body makes (e.g. genotype MZ will have Pi MZ). Exceptions include people on augmentation therapy and who have had a liver transplant. In these cases a normal Pi M is detected due to the treatment and may not correlate with the person’s genes.
The normal Pi type is M. Normal M variants include M1, M2 and M3. Abnormal Pi types included Z, S, F, I and others.
In most cases your Pi type and your genotype are the same since the genes instruct the type of alpha-1 antitrypsin your body makes (e.g. genotype MZ will have Pi MZ). Exceptions include people on augmentation therapy and who have had a liver transplant. In these cases a normal Pi M is detected due to the treatment and may not correlate with the person’s genes.
Who should be tested?
According to the 2016 Guidelines for
The Diagnosis and Management of Alpha-1 Antitrypsin Deficiency in the Adult:
- All individuals with COPD regardless of age or ethnicity should be tested for AATD.
- All individuals with unexplained chronic liver disease should be tested for AATD.
- All individuals with necrotizing panniculitis, granulomatosis with polyangiitis, or unexplained bronchiectasis should be tested for AATD.
- Parents, siblings, and children, as well as extended family of individuals identified with an abnormal gene for AAT, should be provided genetic counseling and offered testing for AATD (see guideline document for special considerations about testing minors).
How can I be tested?
There are several options for getting tested.
-
The Alpha-1 Coded Testing (ACT) Study
is a free and confidential testing program supported by the Alpha-1 Foundation. Testing through this program is voluntary and nobody gets your results except you.
Adults (18 and over) are required to complete their own forms. Parents and legal guardians may complete the forms for their minor children and those in legal guardianship.
-
You may ask your healthcare provider to order testing for Alpha-1. Many labs offer Alpha-1 testing with order from a healthcare provider, including hospital labs, large reference labs, genetics labs, and alpha-1 specialty labs. Different labs may use different testing methods, have different capabilities and limitations, and have different costs associated.
Several Alpha-1 industry partners offer free testing. For example, your healthcare provider can request kits for free testing in healthcare practice through the Grifols AlphaID program.
Talk to your healthcare provider if you have questions about which test is being ordered and details of the test. If your healthcare provider orders your test, the results will go to that healthcare provider to be shared with you, and be part of your medical record.
-
The
Grifols AlphaID At Home
program offers free patient-initiated testing without involvement of a healthcare provider.
- Some direct-to-consumer genetic tests, such as 23andMe, test for common Alpha-1 variants.
What does testing involve?
Alpha-1 testing may be performed on a blood, saliva or cheek swab sample, depending on the test. Blood testing may involve dried blood spots from a finger stick or a blood draw in a doctor’s office. Blood testing is necessary to test AAT level and phenotype and may also be used for genetic testing. Saliva or cheek swab samples can be used for genetic testing and are accepted by some labs and direct-to-consumer genetic testing services.
What does the lab do to test for Alpha-1?
It depends on the lab. There are several ways to test for Alpha-1. Some labs use more than one to ensure accuracy.
An immunoassay, also called a ‘level’, measures the quantity of Alpha-1 in your blood. This is done on one of two scales, either uM or mg/dL, and is reported as a number. This is helpful to see if you have a low level that indicates deficiency.
Phenotyping looks at the Alpha-1 protein(s) in your blood using a technique called isoelectric focusing. The results are two letters called a Pi type, which includes one or two letters (e.g. Pi M, Pi Z, Pi MZ).*
Genotyping spot checks the Alpha-1 gene for specific mutations. The results are two letters called a genotype* or describe whether 0, 1 or 2 mutations were found. Small genotyping tests may look for the S and Z (most common) mutations only, while expanded genotyping panels look for up to 14 variants.
An immunoassay, also called a ‘level’, measures the quantity of Alpha-1 in your blood. This is done on one of two scales, either uM or mg/dL, and is reported as a number. This is helpful to see if you have a low level that indicates deficiency.
Phenotyping looks at the Alpha-1 protein(s) in your blood using a technique called isoelectric focusing. The results are two letters called a Pi type, which includes one or two letters (e.g. Pi M, Pi Z, Pi MZ).*
Genotyping spot checks the Alpha-1 gene for specific mutations. The results are two letters called a genotype* or describe whether 0, 1 or 2 mutations were found. Small genotyping tests may look for the S and Z (most common) mutations only, while expanded genotyping panels look for up to 14 variants.
- Genotyping and phenotyping give you the same result in most cases.
I was diagnosed with AATD. What are the medical recommendations for me?
Please see the 2016 Guidelines at
https://journal.copdfoundation.org/jcopdf/id/1115/The-Diagnosis-and-Management-of-Alpha-1-Antitrypsin-Deficiency-in-the-Adult
and discuss your personal medical recommendations with your healthcare provider.
You should always discuss your personal medical recommendations with a personal healthcare provider.
You should always discuss your personal medical recommendations with a personal healthcare provider.
Is augmentation therapy right for me?
Please see the 2016 Guidelines at
https://journal.copdfoundation.org/jcopdf/id/1115/The-Diagnosis-and-Management-of-Alpha-1-Antitrypsin-Deficiency-in-the-Adult
and discuss your personal medical recommendations with your healthcare provider.
You should always discuss your personal medical recommendations with a personal healthcare provider.
You should always discuss your personal medical recommendations with a personal healthcare provider.
If I have abnormal Alpha-1 gene(s), what else should I do?
Advances in understanding and treating conditions like Alpha-1 are made through research. Consider joining the
Alpha-1 research registry.
AlphaNet
and the
Alpha-1 Foundation
also offer many support resources and medical resources for people affected by Alpha-1.